Keywords: Alcohol abuse, carbohydrate-deficient transferring, γ-glutamyltransferase
CK Wong and CWK Lam
Department of Chemical Pathology,
The Chinese University of Hong Kong,,
Prince of Wales Hospital, Shatin, NT, Hong Kong
Introduction
Alcohol is the most abused drug in the Western world. In the US and Europe, it is estimated that 10 % of the population have medical problems related to alcohol abuse [1]. Six and half percent of Australian adults meet criteria for alcohol abuse disorder [2]. According to WHO, 5 - 6 % of GNP is spent on due to alcohol-related problems, through (1) reduced productivity, (2) accidents and (3) reduced mental and physical well-being. A community study of alcoholism conducted by the Psychiatric Epidemiology Research Unit at the Chinese University of Hong Kong showed that the life-time prevalence of alcohol abuse and/or dependence in Hong Kong was about 9 % in men and less than 1 % in women [3]. Coupled with the growing problem of alcohol abuse, drink-driving offences in Hong Kong have reached a new high [4]. More than 10 % of drivers involved in accidents were found to have consumed alcohol and about 6 % had blood alcohol level greater than 80 mg of alcohol per 100 ml of blood [4]. A recent psychometric analysis of the Alcohol Use Disorders Identification Test (AUDIT) showed that there are indications of increasing alcohol overuse in Hong Kong [5].
Markers of alcohol abuse
γ -glutamyltransferase (GGT)
Although the detection of heavy alcohol consumption and monitoring of its reduction are very important in medical care, it is estimated that only 20 % of heavy consumers of alcohol are identified by their physicians and of these only 20 % are counseled or referred for treatment. γ -glutamyltransferase (GGT) has been used as a highly standardized, easily measurable and inexpensive marker for alcohol abuse. However, it produces false-positive results regarding chronic alcohol abuse in many disease states, e.g. obstructive liver disease, posthepatic obstruction, hepatitis, fatty liver, liver cirrhosis, liver carcinoma with metastases, cardiac insufficiency, mononucleosis, renal transplant, hyperthyroidism, myotonic dystrophy, diabetes mellitus, renal transplant, hyperthyroidism and pancreatitis. Moreover, GGT is highly inducible and affected by several medications e.g. barbiturates, cephalosporins, estrogens, oral contraceptives, phenytoin, primidone, tyrostatics, anabolic steroids, phenothiazines and antirheumatics. Therefore, there is a need for developing other more specific markers for alcohol abuse.
Carbohydrate Deficient Transferrin (CDT)
Transferrin (TRF), the most important iron-transport protein, is synthesized mainly in hepatocytes and consists of three substructural domains: a single polypeptide chain, two independent metal ion-binding sites (within N-terminal and C-terminal domains, respectively), and two asparagines-N-linked complex glycan chains (Fig.1). The human TRF is a glycoprotein with molecular weight of 79.6 kDa. Following serum protein electrophoresis, it is located in the -globulin fraction. About 30 % of TRF is saturated with iron in healthy subjects.
Stibler and Kjellin [6] were the first to report the presence of TRF isoforms with pIs > 5.7 in cerebrospinal fluid and serum of alcoholics. It has been documented that persons with a daily intake of 50 - 80 g of ethanol for one week have detectably elevated asialo-, monosialo-, and disialo-isoforms of transferrins (CDT) (Fig.2) [7]. CDT disappears after abstinence, with a half-life of about 14 days [7].
Pathophysiological mechanism of CDT elevation
The pathophysiology for the increase in CDT isoforms during chronic alcohol abuse is not completely understood at present. It is most likely that ethanol and/or its metabolite acetaldehyde inhibit the initial mannose-dependent steps of TRF N-glycan chain synthesis in the Golgi apparatus of hepatocytes. Sialidase can degrade the sialic acid of the N-glycan chain of transferrin and that sialyl, galactosyl, and N-acetylglucosaminyltransferases are necessary for N-glycan chain synthesis. Xin et al [8] reported increased sialidase activity of hepatocyte and reduced sialyl, galactosyl, and N-acetylglucosaminyltransferases in Golgi homogenates of alcohol-treated rats.
Measurement of CDT
The analysis of CDT makes very high demands on selectivity, specificity, and sensitivity for three main reasons: (a) the distinct serum TRF microheterogeneity; (b) the distinct structural similarity of CDT and non-CDT isoforms; and (c) the low CDT isoform concentrations (< 2.5 - 2.7 % in healthy controls and < 20 % in alcoholics).
Currently there is a paucity of CDT-specific reactions or CDT antibodies, therefore no homogenous CDT assay is available at present. Consequently, routine laboratory analysis of serum CDT requires separation of CDT from other serum proteins and from non-CDT TRF isoforms. This can be performed by chromatographic (e.g. anion-exchange) or electrophoretic [e.g. isoelectric focusing (IEF)] methods, using the different charges and pIs of CDT and non-CDT isoforms. There are coexisting CDT and non-CDT isoforms with almost equal pIs, e.g., disialo-Fe2-TRF (the main CDT isoform), tetrasialo-Fe1N-TRF, pentasialo-Fe1C-TRF (Fig.2). To reduce the number of TRF isoforms occurring in the native serum sample and to preclude coexistence of CDT and non-CDT isoforms with equal pIs, CDT analysis usually starts with in vitro TRF Fe3+ saturation, this treatment establishes a uniform TRF iron load.
1. Electrophoretic method
1.1. Isoelectric focusing
In IEF for the analysis of CDT, the first step is in vitro saturation of TRF with Fe3+. The TRF isoforms are then separated in a gel containing a pH gradient according to their characteristic pIs using electrophoresis. After electrophoresis, the TRF bands are visualized by immunofixation and the CDT-anti-TRF complexes are stained. Finally, the TRF band patterns can be evaluated by densitometry [9].
1.2. Capillary electrophoresis
Capillary electrophoresis and capillary zone electrophoresis have been proposed for the analysis of TRF isoforms. The main problem with these techniques is coating of the capillary surface to prevent protein adsorption and finding a coating-compatible, highly ultraviolet-transparent buffer [10].
2. Chromatographic method
Compared with IEF, anion-exchange chromatographic CDT methods are less sensitive (sample volumes of 100 - 500 ml are required). HPLC method can be used to detect genetic TRF variants in serum from healthy blood donors [11]. However, time-consuming HPLC column regeneration reduces the applicability of HPLC for large CDT analysis series [11]. Recently, lectin affinity chromatography has been used to separate disialo-TRF and asialo-TRF fractions (CDT) from serum [12].
3. Mass spectrometry
Recently, a rapid method for the determination of CDT has been developed using immunoaffinity liquid chromatography and electrospray mass spectrometry [13]. Briefly, serum (25ml) is diluted with 100 ml of water before application to an immunoaffinity column that sequestered TRF isoforms. TRF isoforms are then eluted from the immunoaffinity column, concentrated on a C4 column and eluted before mass spectrometric analysis. Automatic analysis of the CDT isoforms can be completed within 10 minutes [13].
4. Commercial CDT tests
Many commercial CDT tests have been developed since 1993 including CDTect-RIA, CDT-EIA (Pharmacia & Upjohn, Uppsala, Sweden), %CDT-TIA (Axis-Shield, Oslo, Norway), %CDTri-TIA (Bio-Rad Laboratories, CA, USA) and Tinaquant-%CDT/transferrin (Roche Diagnostic GmbH, Germany). The above methods are based on fractionation of CDT and non-CDT isoforms on anion-exchange microcolumns before quantitation of CDT isoforms by immunoassay. In assay kit of %CDT test, total transferrin is determined separately and CDT:total TRF ratio is calculated. The advantage of the CDT:TRF ratio is that it improves the diagnostic specificity of CDT in patients with increased TRF.
Diagnostic specificity and sensitivity of CDT for alcohol abuse
Because of different analytical specificities and recoveries, reference range values for absolute and relative serum CDT are method-dependent (Table 1). Moreover, absolute serum CDT concentrations from healthy women typically are higher than those of healthy men [14, 15]. It is because females frequently have subclinical iron deficiency, which increases TRF concentration and may account for higher CDT concentrations. The main causes for false-positive results in CDT analysis include primary biliray chirrosis, chronically active hepatitis, end stage liver diseases, cystic fibrosis and carbohydrate-deficient glycoprotein syndrom (CDG syndromes). There are several conditions that can affect the diagnostic sensitivity of CDT as marker of chronic alcohol abuse including age, drinking patterns, body mass, hypertension, smoking and sex [16]. However, CDT has fewer sources of false-positives than GGT and is the most specific laboratory marker of chronic alcohol abuse.
Conclusions
The analytical performance, specificity, sensitivity and reference interval of CDT analysis have to be further standardized because of different existing analytical methods. Moreover, CDT is not a screening tool for detection of increased alcohol consumption but the most specific marker of chronic alcohol abuse. Diagnosis of chronic alcohol abuse should always be made based on a clinical background, questionnaire, CDT, GGT, and not on a single CDT value. Further efforts have to be made for a uniform definition of CDT and standardization of CDT analysis.
Reference
Fig.1 Structure of serum iron transport
protein human transferrin.
Fig.2 Microheterogeneity of human serum
TRF attributable to various TRF-Fe3+ loads and different N-glycan
chains. The percentage is the % of each isoforms in healthy subjects.
| Pentasialo-Fe1C- Transferrin (12 - 18 %) |
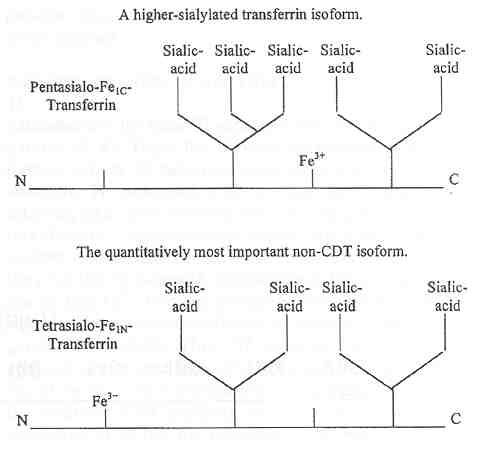 |
| Tetrasialo-Fe1N- Transferrin (64 - 80 %) |
| Trisialo-Fe0- Transferrin (4.5 - 9 %) |
 |
| Disialo-Fe2- Transferrin (< 2.5 %) |
|
Asialo-Fe2- Transferrin (< 0.5 %) |
Table 1.
Some reference values of serum CDT using different methods [16]
| Method | Women | Men |
| CDTect-RIA | 26-28 units/L | 26-28 units/L |
| CDTect-EIA | 26-28 units/L | 18-20 units/L |
| %CDT-TIA | 5-6 % | 5-6% |
| Capillary zone Ep | < 3 % | < 3 % |
| HPLC | 80 mg/L | 80 mg/L |
| IEF-Immunofixation | < 4.4 % | < 4.4 % |
| IEF-Western blotting | 100 mg/L | 100 mg/L |
| Lectin affinity chromatoragphy | < 1.3 % | < 1.3 % |